

STRATEGIC TRANSFORMATION PLANS
WHAT NEEDS TO BE DIFFERENT THIS TIME

STPs - The Mystery of 'What, Why and How'. A marking guide for STP assessors
Over the next few weeks 44 Strategic Transformation Plans (STPs) will be pored over and 'marked' by NHS England and NHS Improvement.
So what needs to be different this time? What will give us any more confidence that we have this time solved the mystery of implementation - making the linkages between 'Why', 'What' and 'How'. I suggest both STPs and their assessors will need to discard some well entrenched orthodoxies.

Over the next few weeks 44 Strategic Transformation Plans (STPs) will be pored over and 'marked' by NHS England and NHS Improvement.
The NHS has been here many times before. There is a lot of expensively drafted history gathering real and virtual dust on many bookshelves of organisations, many of which exist only in the memory of the consultants who were paid a lot to write such things. So what needs to be different this time? What will give us any more confidence that we have this time solved the mystery of implementation - making the linkages between 'Why', 'What' and 'How'. I suggest both STPs and their assessors will need to discard some well entrenched orthodoxies.
Why
What we might expect to find: An elegant and convincing exposition of the 'Why' replete with socio-demographic projections, public health prognostications, activity analysis and expenditure trends models linked, workforce analysis, funding gaps explored and obeisances made to the Five Year Forward View all packaged as an irrefutable case for change.
But how many STPs will acknowledge that the analysis is only as current as the date of writing (not even of printing) - that 'events' may yet fundamentally change the emphasis and priorities? What is said about how the 'Why' is continually reviewed and refreshed, how existing scenarios are continually updated and new scenarios developed, how changes in direction and priority are decided and how people understand that anticipating potential futures is not about being indecisive but being prepared?
How many STPs have modelled Brexit as a possibility? How many on submitting the plans last week will have included the caveat that the plan is now out of date and they will now have to revise it to include the Brexit scenario? Or are they just waiting to be given a new set of assumptions?
What
What we might expect to find: A detailed prescription of the 'What' without doubt including one of those delightful concentric ring diagrams with patients and carers comfortingly at the centre. There will be detailed integrated care models, proposals for service reconfiguration, matrices, flow diagrams, heroic savings projections and trajectories, and lots to say about patient safety, quality and engagement. Vanguards will be quoted and there will be lots to be said about 'New Models of Care' - which in truth are not new but it is just that we have failed to find a way of implementing them so far.
How many STPs will be honest enough to acknowledge that 'no plan survives first contact with reality' and that what the system eventually ends up looking like might be very different from what was originally described. That the journey needs to be one of constant learning from a mixture of success and failure and adjusting accordingly. That change is a process of relentless exploration, making and taking opportunities and being brave enough to acknowledge failure and dead-ends and rapidly looking for alternatives. How many acknowledge that the biggest risk is not failure but the need to succeed at any cost?

The risks of the need to succeed at any cost
How
And then we come to 'How' all of this will be achieved? And this is where history has a lot to teach us - not least that we would probably not be in this position now if we had managed to systematically sort out the 'how' in any of our previous NHS incarnations.
What we might expect to find: An elegant but busy governance structure diagram with Programme Boards, Committees, Locality Groups, Enabling Workstream Groups, Programme Offices and all the other bureaucratic paraphernalia. These structures are often a dense scaffolding confection that contains little more than thin air or platitudes - and moreover miraculously appear in mid-air built downwards. These structures will usually have a costed 'Programme Office' but will largely ignore the input costs of the time of those required to prepare for and attend the myriad of meetings and make no mention of the opportunity costs imposed because they are not running their own organisations and keeping today's business on the road. There will probably be little or no mention of the modern digital infrastructure that will support the process.
How many of these STPs will have a single coherent model of change at the core of the 'How'? How many of the platitudes of co-design, co-production, leadership, shared purpose, team building and workforce development will be given backbone by a simple clear description of how front-line teams will tackle the challenges they are being set? Is there a clearly described, core system-wide change methodology that will be used consistently by every team and organisation (there is a place for a nice process diagram here - and here is an introduction to one I did earlier!)? What are the core capabilities and capacities that front-line teams - the 'Poor Bloody Infantry' of change - require to deliver this Standard Operating Procedure (SOP) for change and how will this be developed?
Is the governance structure built from the ground-up as an enabling scaffolding for front-line teams - one that aligns with the single coherent model of change and that actually embodies in the way it conducts business the flexibility, agility and rapid learning that characterises successful and energetic change? Is the cost of the governance structure worth it and indeed why would anybody want to bother turning up after the first two interminable meetings?
Is there a modern digital collaboration infrastructure in place to support the front-line teams and the programme as a whole - or is it email and attachments as usual? Was it even used to develop the STP in the first place?
So the challenge for both STPs and those assessing them:
If you always start from where you have always started, do not be surprised if you end up where you have always ended up, feeling much as you have always felt.

Changing culture one habit at a time
If we accept that, as individuals, we are the culture then our mental model shifts to see organisational culture as an accumulation of individual habits that become aligned and ingrained over time. In this mental model the first and biggest shift for any effort to change culture is the acceptance by each individual within the organisation that 'I am the culture'...
NHS Improvement recently announced that it was working with the King's Fund on 'a two-year programme to help NHS providers develop cultures that enable and sustain continuously improving, safe, high quality, compassionate care'.
I have nothing against this per-se although I do wonder why we need another culture diagnostic and change programme when there are so many already out there - just Google it and see the wealth of resources already available. Which inevitably brings us to the question which is 'why this one will be any more effective than any of the others'.
What is central to the successful delivery of a 'culture change' programme is the mental model we hold in our minds when we discuss organisational culture.
Just as we tend to anthropomorphise animals we are often at risk of anthropomorphising the inanimate when we talk about culture - in this case organisations. An organisation is not an animate entity, an animal or a plant or even a person. An organisation is 'simply' a framework within which individuals are 'organised'. Individuals are the culture.
Too often when we blame organisational culture our mental model reinforces the transfer of the responsibility and the focus of the culture away from ourselves to something that is 'other than us'- to the organisation. As a result we take on a victim mentality where culture is seen as a dragon to be slain - a Smaug coiled around the jewels of our enterprise stifling it and preventing us fulfilling our potential. This naturally leads to the search for a 'dragon slayer' - and a great deal of tilting at windmills (to mix a number of literary allusions). Many approaches to cultural change risk perpetuating this mentality. Culture becomes a SEP - a Somebody Else's Problem.

Definitely would prefer this one to be an SEP
If we accept that, as individuals, we are the culture then our mental model shifts to see organisational culture as an accumulation of individual habits that become aligned and ingrained over time. In this mental model the first and biggest shift for any effort to change culture is the acceptance by each individual within the organisation that 'I am the culture - my habits positive, negative, and coping contribute to what we are collectively'.
In this model the first step to changing culture is for individuals to take personal ownership of the challenge; to identify the personal habits that need to be challenged - identifying those that should be given more emphasis and others that need to be replaced with new habits.
At this stage we need to ground our understanding in terms of the cost to ourselves, our patients/clients and to our colleagues of not changing our habits. And then we need to select the one habit to start with - the one personal change that allows us to begin the journey, which, when added to all the other personal experiments in the organisation begins to unlock wider potential and begin the cultural shift.
The role of leaders throughout an organisation is to role model this themselves - to lead the way, to break through their own Self Limiting Assumptions, to be the change they want to see in others and to provide the support, permissions and space for others to do the same.
So what is the habit you are going to change first/next?
Culture changes one habit at a time

The Interoperability Fallacy in Health and Social Care - what about ‘Me'?
Lets be clear - your data is not about me. Its about the things you do to parts of me. It is the stuff that matters to you because it is your everyday business - I give you that, but it is not about the real me. It might be a ‘patient record’ but it sure as hell is not a ‘me’ record.
I have just been listening to a group of senior NHS and Social Care staff lamenting the lack of interoperability of their IT systems.
So lets just get this one in - what about the interoperability of your systems with me - the patient/user?
Lets be clear - your data is not about me. Its about the things you do to parts of me. It is the stuff that matters to you because it is your everyday business - I give you that, but it is not about the real me. It might be a ‘patient record’ but it sure as hell is not a ‘me’ record.
Allowing me a view into the data you hold on me is all very kind and no doubt allows the government to tick a policy box somewhere but it is usually incomprehensible in the context of the real me.
So let’s be crystal clear - what I want is for your systems to be interoperable with me.
Think about it for a moment - it might make life a whole lot easier for you than it is now. If you need to make all your systems interoperable with each other think of the number of different connections you have to make and the different standards that have to be navigated. And I bet it will make it even more complicated for patients/users.
So I want a 'Me Record'. You are holding bits of the jigsaw of data about me and I require you to make it available to my ‘Me Record’. I can add whatever else I think is important whenever I want - my Fitbit data, telecare data, my shopping habits, my Living Will, my ambitions for a life well lived.
I will decide who I make it available to - I am best placed to make the risk/benefit decision about sharing (perhaps with some good advice), not some risk-averse NHS or Social Care organisation being anally retentive about security and confidentiality to the detriment of my care. I might want to make it available for research, or have it send alerts to my family or GP. I might even want to sell my data - why not?
And just to anticipate your comments about inequality of access to the internet etc - well by the time you get your combined acts together there will be a whole generation of Baby Boomers who have grown up with using the internet for everything from shopping to banking to booking holidays. There will be more than enough of them to act as early adopters, pathfinders exploring the route for those that follow. Enough to make a difference to the way you design and deliver services, enough to make integrated service delivery a lot easier - provided of course that is what you really want for me.
So - make your systems interoperable with me please. It might make everybody’s life a lot easier.
An Agile Manifesto for NHS improvement and redesign
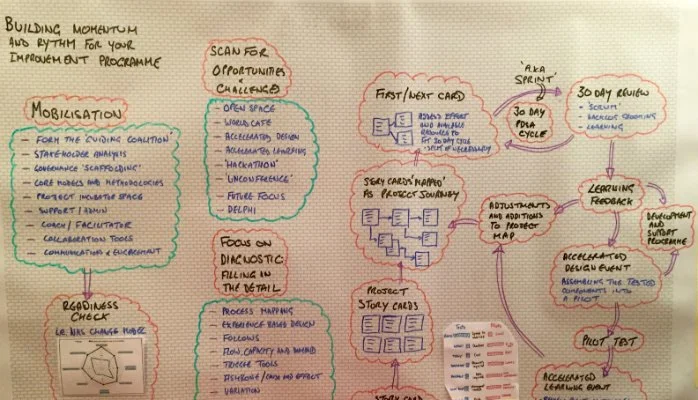
I have been working in quieter moments to begin to translate those original Agile concepts and methodologies to the world of service improvement within the NHS. As part of this I assembled a number of bits of a jigsaw to help me 'triangulate' and then sketched out the bones of the idea on a whiteboard.
About 14 years ago a group of software developers got together at a ski resort in the US to find an alternative to the top-down, over-bureaucratic and over-documented approaches to software development that were a feature of programming at the time. Many of them were already 'insurgents' experimenting with new development techniques that were better suited to the rapidly changing technology landscape.
Out of this came a bigger, international, gathering of like-minded individuals and the development of the Agile Manifesto. This was the beginning of a movement that in time has seen the development of methodologies that have transformed the time it takes to get software from concept to delivery and that have transformed the pace at which software is updated and released.
I have translated the manifesto (it was not difficult) into an Agile Manifesto for NHS 'improvers'

I have been working in quieter moments to begin to translate those original Agile concepts and methodologies to the world of service improvement within the NHS. As part of this I assembled a number of bits of a jigsaw to help me 'triangulate' and then sketched out the bones of the idea on a whiteboard. Three other images form part of the jigsaw with thanks to @PaulBromford (Paul Taylor at Bromford labs) for the Tests and Pilots diagram and @whatsthepont (Chris Bolton) and to IHI amongst many others for the Model for Improvement.
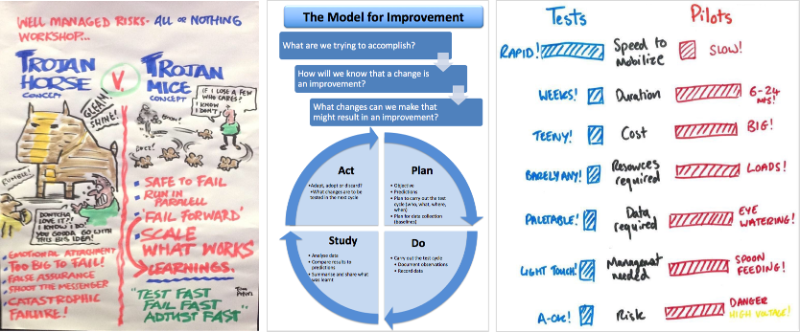
So here is the journey around my whiteboard